

Multiple sclerosis. MS is an autoimmune disease in which the immune system attacks the protective myelin that covers nerve fibers. MS has a disabling effect on communication between the brain and central nervous system and and the rest of the body. There seems to be a role for Coenzyme Q10 in the treatment of multiple sclerosis.
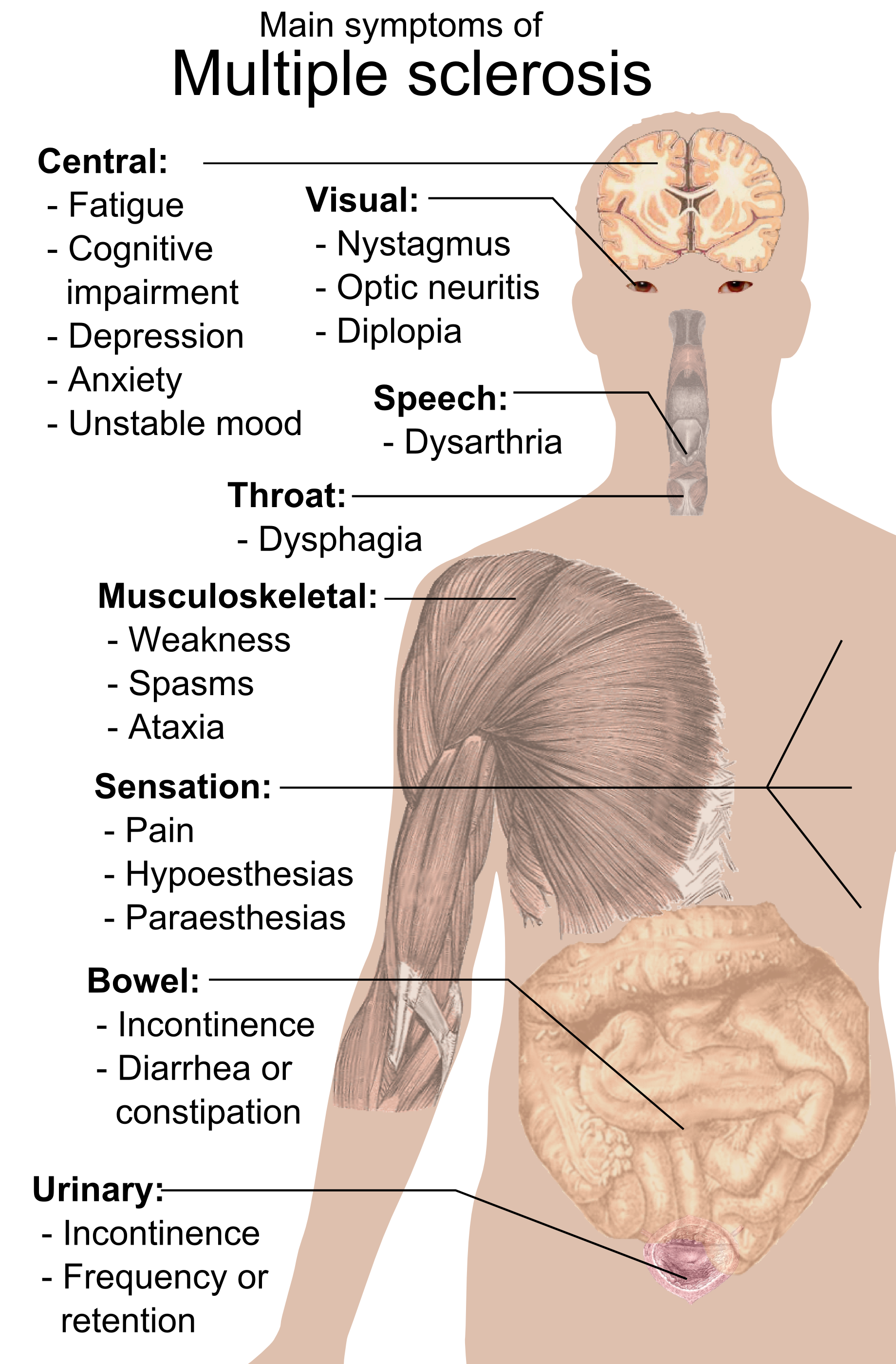
There is a rationale for the use of supplemental Coenzyme Q10 as a therapeutic agent for multiple sclerosis, given the key roles of Coenzyme Q10 in normal mitochondrial function, in antioxidant defense, and in anti-inflammatory action. David Mantle and Iain Hargreaves have reviewed the relevant research literature. Attribution: Mikael Häggström, Public domain, via Wikimedia Commons.
Adequate levels of Coenzyme Q10 are needed for normal mitochondrial function, for antioxidant defense, and for protection against inflammation. Mitochondrial dysfunction, oxidative stress, and inflammation are all factors in the development and progression of MS [Mantle 2023].
Note:
- For normal functioning, cells depend upon ATP energy generation in the mitochondria.
- Oxidative stress is defined as an imbalance between the damaging effect of free radicals and the action of free radical neutralizing antioxidants such as Coenzyme Q10.
- Inflammation is both a positive immune system process necessary for a response to infection and injury and a negative process when it involves the release of pro-inflammatory cytokines.
A review of the relevant research literature shows that there can be a rationale for the use of supplemental Coenzyme Q10 as a therapeutic agent in MS [Mantle 2023].
Importance of Coenzyme Q10
Coenzyme Q10 is not a vitamin – it is synthesized in almost all cells in the body – but it does has vitamin-like properties. The highest levels of CoQ10 biosynthesis occur in our 20s. Thereafter, with increasing age, the endogenous synthesis of Coenzyme Q10 declines. It declines to the extent that the synthesis of Coenzyme Q10 in heart muscle tissue is only 50% at age 80 as it was at age 25 [Kalén 1989].
In the cells and tissues, Coenzyme Q10 exists in both an oxidized form called ubiquinone and a reduced form called ubiquinol. There is a continuous conversion back and forth between these two forms, depending upon need [Mantle & Dybring 2020].
Relevance of Coenzyme Q10 for MS Patients
As indicated above, Coenzyme Q10 plays three important roles that suggest a potential relevance to the treatment of multiple sclerosis:
- Inside the mitochondria, Coenzyme Q10 plays an essential role in the process of ATP energy generation [Mantle & Dybring 2020].
- Coenzyme Q10 is an important lipid-soluble antioxidant that protects cells against oxidative stress. Coenzyme Q10 is the only lipid-soluble antioxidant that is synthesized endogenously [Mantle 2023].
- Coenzyme Q10 seems to affect the expression of several genes, including genes involved in inflammation [Mantle 2023].
Evidence for Coenzyme Q10 in MS Treatment
- There is evidence that MS patients’ blood levels of Coenzyme Q10 are significantly below the levels of normal healthy controls [Mantle 2023].
- There is evidence from clinical trials that shows that CoQ10 treatment of MS patients results in reduced levels of oxidative stress and inflammation, reduced fatigue symptoms, and reduced risk of depression [Sanoobar 2015].
Bioavailability of Coenzyme Q10
The success or failure of CoQ10 treatment of MS patients will depend upon the extent to which the supplemental Coenzyme Q10 is absorbed and available for uptake in the cells and tissues. Because the CoQ10 raw material is a crystalline powder and because CoQ10 molecules are large, lipid-soluble molecules, absorption is typically quite low, 5% or less, perhaps 6-8% in the best supplement formulations. The CoQ10 crystals must be dissolved to single CoQ10 molecules at body temperature for absorption to take place [Mantle 2023].
In a randomized controlled clinical trial, Lopez-Lluch et al tested seven CoQ10 supplements with differing formulations in the same group of 14 healthy individuals. The researchers used a crossover/washout protocol. They measured the bioavailability of the different formulations as the area under the curve at 48 hours [Lopez-Lluch 2019].
Lopez-Lluch and the research team found that the CoQ10 ubiquinone supplement formulation that had been subjected to a patented crystal modification process had the highest level of bioavailability [Lopez-Lluch 2019]. The ubiquinone test product had double the bioavailability of a ubiquinol test product. This outcome shows that the formulation of the CoQ10 supplement is more important to CoQ10 absorption than is the form of the Coenzyme Q10, i.e., whether ubiquinone or ubiquinol.
Safety of CoQ10 Supplements
Clinical trial data indicate that the observed safety level for Coenzyme Q10 is 1200 mg/day/person. Pharmacokinetic studies have shown that CoQ10 supplementation does not influence the biosynthesis of endogenous Coenzyme Q10 and does not cause Coenzyme Q10 to accumulate in the plasma or the tissues after the cessation of supplementation. Overall, data from preclinical and clinical studies indicate that CoQ10 supplementation is highly safe [Hidaka 2008].
No serious adverse effects have been reported in any of the 400 randomized controlled clinical studies reported in the medical literature. On very rare occasions, individuals may experience mild gastrointestinal disturbance [Mantle 2022]. In the Q-Symbio clinical trial of adjuvant CoQ10 supplementation of chronic heart failure patients, there was no significant difference in adverse events between the CoQ10-treated group and the placebo group over the
course of the two-year study [Mortensen 2014].
There are no known toxic effects. Coenzyme Q10 cannot be overdosed (Hidaka 2008).
Sources
Häggström, Mikael (2014). “Medical gallery of Mikael Häggström 2014”. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.008. ISSN 2002-4436. Public Domain.
Hidaka T, Fujii K, Funahashi I, Fukutomi N, Hosoe K. Safety assessment of coenzyme Q10 (CoQ10). Biofactors. 2008;32(1-4):199-208.
Kalén A, Appelkvist EL, Dallner G. Age-related changes in the lipid compositions of rat and human tissues. Lipids. 1989 Jul;24(7):579-84.
López-Lluch G, Del Pozo-Cruz J, Sánchez-Cuesta A, Cortés-Rodríguez AB, Navas P. Bioavailability of coenzyme Q10 supplements depends on carrier lipids and solubilization. Nutrition. 2019 Jan;57:133-140.
Mantle D, Dybring A. Bioavailability of Coenzyme Q10: An Overview of the Absorption Process and Subsequent Metabolism. Antioxidants (Basel). 2020 May 5;9(5):386.
Mantle D, Turton N, Hargreaves IP. Depletion and supplementation of Coenzyme Q10 in secondary deficiency disorders. Front Biosci (Landmark Ed). 2022;27(12):322.
Mantle D & Hargreaves IP. Multiple sclerosis: is there a role for Coenzyme Q10? British Journal of Neuroscience Nursing. 2023;19(Sup3):S21-S25.
Mayo Clinic Staff. Multiple Sclerosis. Mayo Clinic. 2023. Retrieved from https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269
Mortensen SA, Rosenfeldt F, Kumar A, Dolliner P, Filipiak KJ, Pella D, Alehagen U, Steurer G, Littarru GP; Q-SYMBIO Study Investigators. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: results from Q-SYMBIO: a randomized double-blind trial. JACC Heart Fail. 2014 Dec;2(6):641-9.
Sanoobar M, Eghtesadi S, Azimi A, Khalili M, Khodadadi B, Jazayeri S, Gohari MR, Aryaeian N. Coenzyme Q10 supplementation ameliorates inflammatory markers in patients with multiple sclerosis: a double blind, placebo, controlled randomized clinical trial. Nutr Neurosci. 2015 May;18(4):169-76.
The information presented in this review article is not intended as medical advice and should not be used as such.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment